SummaryThis is a brief approach to a Colles' Fracture. We begin by discussing the definition of a Colle's fracture with its classical presentation. We then discuss the characteristic radiological features and management.
Definition
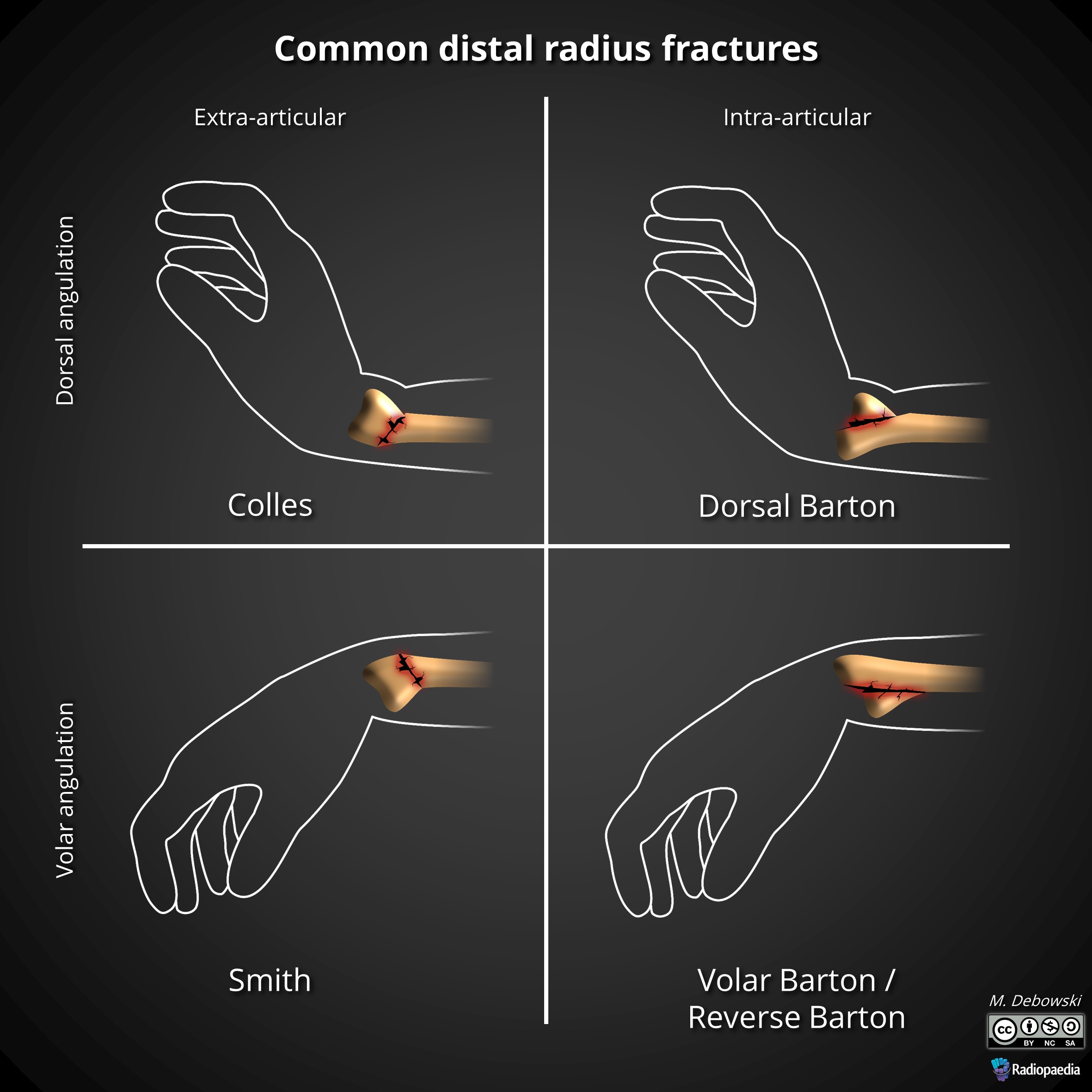
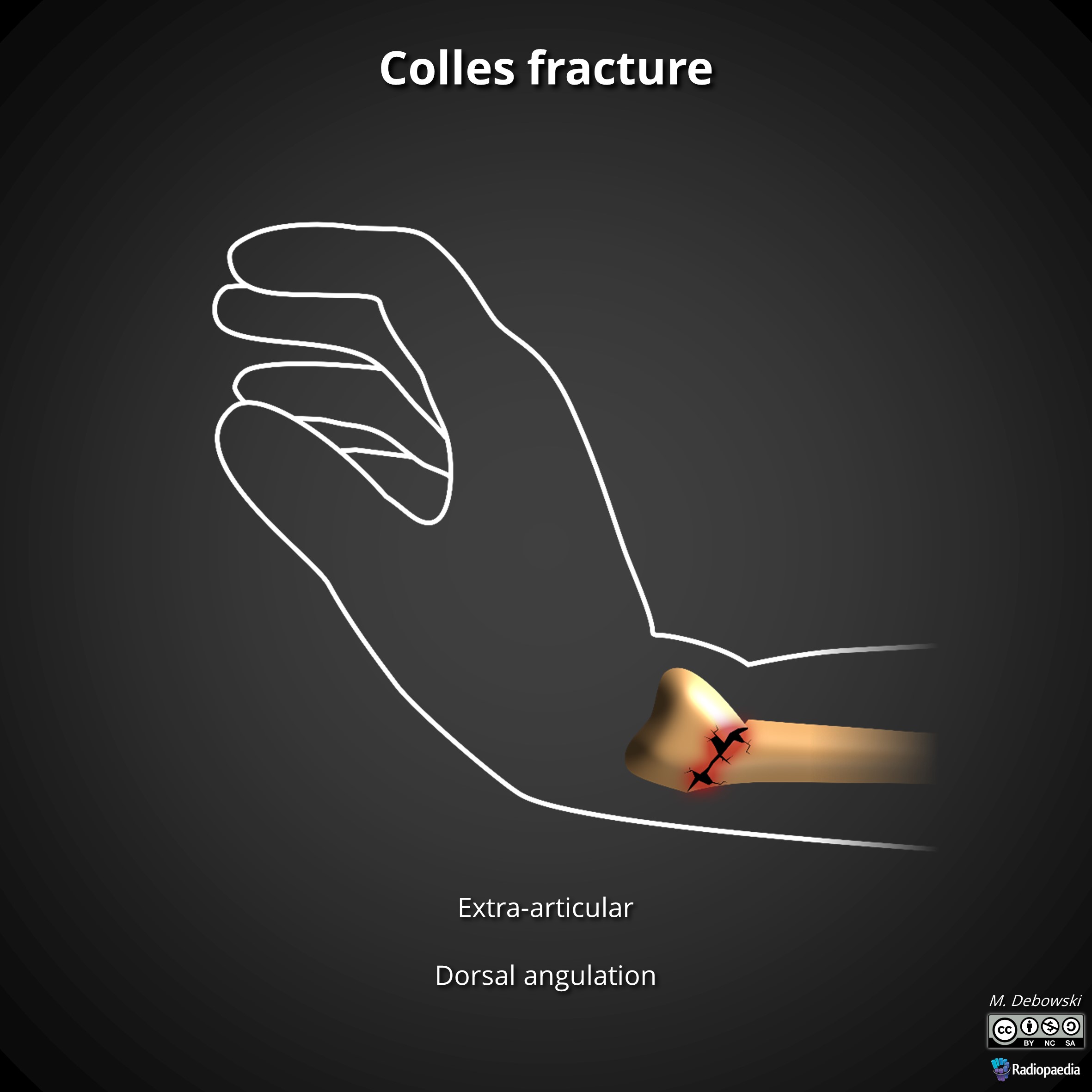
This type of fracture is often described as being an extra-articular transverse fracture of the distal radius with dorsal displacement with/without ulnar styloid fracture. The fracture is usually around 2cm proximal to the radiocarpal joint.
This fracture commonly occurs in patients which have osteoporotic bones (age > 40 years old). The main mechanism of injury is falling on an outstretched hand (FOOSH).
Presentation
Dinner Fork Deformity
Swelling, Ecchymosis, Tenderness
Painful range of motion (ROM)
Investigations
Apart from basic investigations, we focus on the radiographic investigations.
X-Ray: AP and Later x-rays of the wrist. Oblique views of the wrist may also be beneficial. The radiological features include:
Aim1. To restore normal anatomy: Restore radial height (13mm), Radial Inclination (22 deg) and volar tilt (11 deg).
2. To restore or regain full function of the wrist and hand.
Non-Surgical
Procedure: Closed reduction with a haematoma block or conscious sedation. For the closed reduction, you should apply traction with hyperextension of the distal fragment (exaggerates the injury), then traction with ulnar deviation. Pronate then flex the distal fragment.
After closed reduction, apply a dorsal slab (because of too much swelling) or a below elbow cast for 6 weeks. The wrist should be maintained in a slight flexion position.
Get post reduction x-rays immediately and review, repeat the reduction if it is necessary to do so. Features that suggest failed closed reduction:
Radial Shortening > 3 mm post reduction or
Dorsal tilt > 10 deg or
Intra-articular displacement > 2mm
NB: These patients will benefit from ORIF
If a dorsal slab was used, these patients should be reviewed after 1 week in order to assess that the reduction has been maintained and this slab is changed to a circular cast. The patient is then reviewed after 6 weeks and the cast is removed.
Surgical
Indication:
Displaced intra-articular fracture
Comminuted fracture
Severe osteoporosis
Dorsal angulation > 5 deg or volar tilt > 20 deg
>5mm radial shortening
Failed closed reduction
Loss of reduction after a
Methods:
Percutaneous pinning, Open Reduction and Internal Fixation (ORIF with dorsal or volar plating) or external fixation.
Complications
Early Complications: Difficult reduction, loss of reduction, compartment syndrome, tendon rupture (EPL), acute carpal tunnel syndrome, complications of having a tight casts.