An Approach to a Miscarriage
Defintion
Classification
- Onset
- Spontaneous: Occurs without medical or mechanical intervention
- Induced Abortions
- Clinical
- Threatened:
- Inevitable
- Incomplete
- Complete
- Non-viable pregnancy
- “Missed Miscarriage “: If there is a developed embryo or fetus present on ultrasound but it is dead.
- “Anembryonic pregnancy”: If there is no embryo that has developed within the gestational sac.
- Other
- A miscarriage may also be classified according to the timing (first trimester, second trimester miscarriage) and also on the frequency of the miscarriage (recurrent miscarriage). This has important clinical sign.
Presentation
Products of Conception Passed
The history usually includes symptoms of per vaginal bleeding associated with a several weeks of amenorrhea. The patient may even mention that they have seen some products of conception, including statements such as seeing a “fetus”, “placenta”, or some “fleshy tissue”. In this case, if the cervix is already closed and the uterus appears empty then it suggests a complete miscarriage. Because we are saying that the uterus is empty, we should also ensure that there is no ectopic pregnancy. The patient would still test “positive” in a pregnancy test. If the cervix is still open then the patient might be having an incomplete miscarriage.
No Products of Conception Passed
If there is no passage of products of conception, then the miscarriage may either be a threatened miscarriage or a missed miscarriage. If the patient has some abdominal pains and/or per vaginal bleeding with a closed cervix we call this a threatened miscarriage. A missed miscarriage is technically a miscarriage that is discovered while the patient has no symptoms: There is a dead embryo or fetus but with no symptoms.
Complicated Miscarriage
It is important to ensure that the health care professional actively seeks for signs of a complicated miscarriage. A complicated miscarriage will need a more extensive management and it will include active resuscitation of the patient. Signs of a complicated miscarriage:
- Abnormal vitals
- Systolic blood pressure < 90mmHg
- Respiratory Rate > 20 bpm
- Temperature > 37.5 degrees Celsius
- Haemoglobin < 10 g/dl
- Signs of sepsis or infection
- Fever, Foul smelling products, raised inflammatory markers
- Signs of organ dysfunction
- Altered mental status
- Signs of shock
- Oliguria
Investigations
- Bloods
- Formal Bloods, including B-HCG (qualitative and quantitative).
- The B-HCG levels should double every 48 hours in a viable pregnancy
- Rh status: This is important because all women who have a blood type that is Rh(D) negative and suffered an early pregnancy loss and have not yet been senstitized then they should receive Rh(D) immune globulin to prevent alloimmunisation.
- Blood gas, especially if suspect a complicated miscarriage.
- Cross Match (if necessary)
- Formal Bloods, including B-HCG (qualitative and quantitative).
- Urinalysis and urine pregnancy test
- Imaging
- Ultrasound
- B-HCG:
- B-HCG between 1000 to 2000 UI/I: Transvaginal US (TVUS) is the most sensitive.
- B-HCG between 800 to 1500 UI/I: A 1-3mm gestational sac should be visible by TVUS.
- B-HCG between 4500 to 7500 UI/I: A yolk sac should be detectable.
- B-HCG between 8650 to 12200 UI/I: Fetal heart motion should be visible.
- Others
- At a Crown-Rump Length (CRL) of ≥5mm, cardiac activity should be identifiable.
- B-HCG:
- Ultrasound
Management
Most of the management options can be broadly divided into expectant management, medical and surgical interventions. The surgical intervention refers to the usage of either sharp curettage or suction curettage. In cases where the patient has extensive bleeding, hemodynamic instability or signs of infection then surgical evacuation is preferred. If there are any other complications, surgical intervention is often preferred.
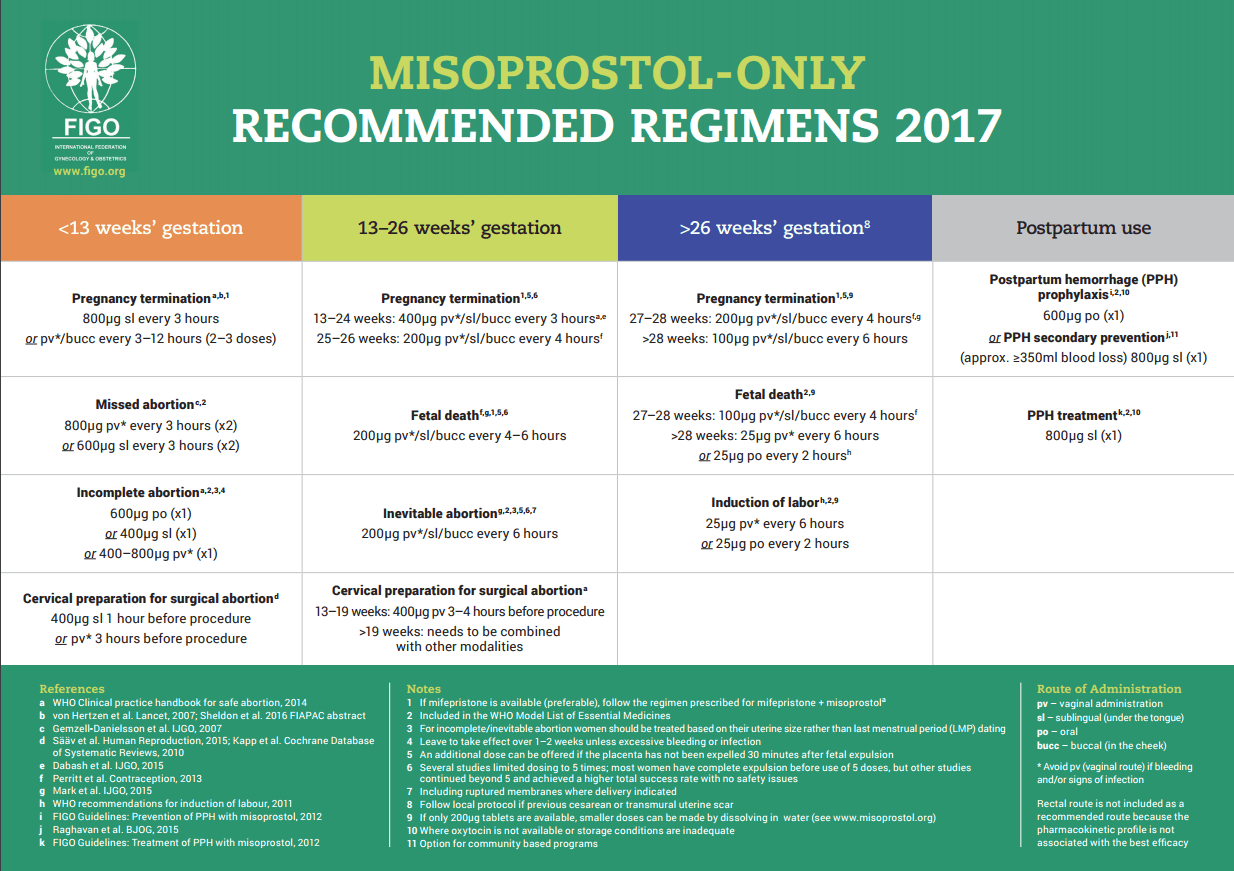
Below we used the Misoprostol dosages recommended by the National Department of Health in the Guidelines for Maternity Care in South Africa (2015). Therefore, do not let this difference in dosages confuse you.
Threatened Miscarriage
In a threatened miscarriage, there is usually mild bleeding without cervical dilatation. The uterus size corresponds to the expected gestation. The transvaginal ultrasound shows a viable fetus.
- Reassure the patient: If the patient’s fetal heart is active then it is stated that the pregnancy has a good chance to continue.
- It is not necessary to admit the patient to the hospital. The patient should be discharged to go home. The patient should be advised to avoid strenuous activity and any sexual activity as well.
- If the bleeding stops, the patient can continue her ante-natal clinic visits as scheduled.
- However, if the pain or bleeding continues, the patient should come return to see a health care practitioner skilled with ultrasound examination.
Complete Miscarriage
In a complete miscarriage, there is usually mild bleeding with a closed cervical os. Because the patient has expelled the products of conception, the uterus may also feel smaller than expected. Remember, transvaginal ultrasound will show an empty uterus and hence one should always look and rule out an ectopic pregnancy. The endometrial thickness on TVUS is usually < 5mm after dilatation and curettage or spontaneous abortion: if it is thicker consider retained products of conception.
- Educate about the current condition
- There is usually no need for medical or surgical evacuation of the uterus.
- Discharge the patient if she is stable and advice the patient that she should return if there is continuous bleeding. She may benefit from post-miscarriage follow-up.
- NB: Ensure that this is indeed a complete miscarriage
Inevitable Miscarriage
This occurs when a threatening miscarriage continues to progress, the cervical os opens (dilates) and the patient begins to bleed more. The patient will also begin to have more cramping pains. On the transvaginal ultrasound there may be either a viable fetus or not.
- If the pregnancy is less than 16 weeks:
- Plan for evacuation of the uterus
- If the evacuation is not immediately possible: Give Misoprostol 400ug PO, then arrange for evacuation of the uterus as soon as possible.
- If the pregnancy is more than 16 weeks:
- Wait for the spontaneous expulsion of the products of conception
- If on inspection, it appears that there products are incomplete then evacuate the uterus to remain any remaining products of conception.
- If necessary infuse oxytocin 20 IU in 1L of Normal Saline or Ringers Lactate over 8 hours (125ml/hour) to help achieve the expulsion of the products
Book the patient for post-miscarriage follow up.
Incomplete Miscarriage
In this case, the patient only passed a portion of the products of conception. For this reason, the cervix remains open with products of conception still visible or felt. The uterus does not correspond to the gestation.
- If the pregnancy is less than 16 weeks:
- If the patient has light bleeding, one may attempt to remove the visible products of conception with the fingers or a swab holding forceps and then observe the patient. If the bleeding then remains light, no further action needs to be taken.
- If the patient has heavy bleeding after remove of the products of conception, this patient will benefit from a uterine evacuation.
- If the evacuation is not immediately possible, give Misoprostol 400ug PO to reduce the risk of bleeding while arranging for the evacuation.
- If the uterus size is < 12-14 weeks, then the preferred method to evacuate the uterus is manual vacuum aspiration (MVA). Only if MVA is not possible or available, then sharp curettage may be used.
- If the pregnancy is greater than 16 weeks:
- The chances that complete spontaneous expulsion occurs is greater, to assist this expulsion.
- Set up an IV line with Oxytocin 20 IU in 1L of Normal Saline or Ringers Lactate every 8 hours (125ml/hour) until the expulsion of the products occur. This patient may benefit from Misoprostol 200ug PO 4 hourly (max 800ug) if the abortion does not progress on oxytocin.
- After the expulsion, examine the uterus and evacuate any remaining products of conception.
- The chances that complete spontaneous expulsion occurs is greater, to assist this expulsion.
Pain Management
Non-steroidal anti-inflammatory drugs (NSAIDs) should be the first line treatment. One should note that NSAIDs do not appear to decrease the action of misoprostol or mifepristone in clinical trials, despite the theoretical concerns about them.
Post-Miscarriage Follow Up
- Counsel the patient about her current condition. Explain that miscarriages are common and unless there was any complications, the chances for a subsequent pregnancy are good.
- The patient should only consider a future pregnancy once she has recovered from her current miscarriage.
- Screen for other clinical conditions: Anemia, HIV status
- Rh status: Rh(D) negative women should receive 50mcg (or 300mcg if available) of Rh(D)-immune globulin to prevent alloimmunisation. This should be done within 72 hours of diagnosing the miscarriage and immediately after a surgical intervention.
- Counsel the patient on family planning and the methods available to her: Hormonal pills, injections, implants, intrauterine contraceptive devices (IUCD) and tubal ligation may be provided immediately to the patient. An IUCD should be delayed if the patient has an anemia < 7 and if an infection is suspected.
- Patient should be counseled for a pap smear either on her return for a follow up or at local clinic.
Notes
- Some health care practitioners prescribe antibiotics in incomplete miscarriages. This is mainly indicated in septic miscarriages and it usually includes:
- Ampicillin 1g IV 6 hourly AND Metronidazole 400mg PO 8 hourly. Instead of Ampicillin one may also use cephalosporin and if the patient is allergic to penicillin one may use Clindamycin 600mg IV 8 hourly.
- Hormone administration has not been proven.
- Anticoagulants and Aspirin has only been proven to benefit patients with antiphospholipid syndrome.
- Misoprostol, is a synthetic prostaglandin that has uterotonic and cervical softening effects. It is much cheaper than Mifepristone. The use of mifepristone in management of early pregnancy loss is debatable. Mifepristone is an anti-progestogen, which increases the sensitivity of the myometrium to prostaglandins by around 5 times with maximal effect on uterine contractility and cervical ripening at 36–48 hours following treatment. This is the reason it is sometimes combined with Misoprostol.
- The dose of misoprostol needs to be modified according to gestational age. This is because the sensitivity of the uterus to prostaglandins increases with increasing gestation.
2. Dugas, C. and Slane, V., 2022. Miscarriage. [online] Ncbi.nlm.nih.gov. Available at: https://tinyurl.com/2udbpu7y [Accessed 24 September 2022].
3. Saraswat, L., W Ashok, P. and Mathur, M., n.d. [online] Elearning.rcog.org.uk. Available at: [Accessed 24 September 2022].
4. Early Pregnancy Issues for the MRCOG and Beyond, 2011. Miscarriage. [online] pp.15-31. Available at: https://tinyurl.com/5x5najzn [Accessed 24 September 2022].


Made with ❤️ by QuickBeat
We are a small education agency that aims to provide medical education.
EXPLORE
SERVICES
CONTACT
- Pretoria North, Gauteng
- contact@quickbeat.co.za