Diuretics and CKD
Summary
This is a summary on how to use diuretics in chronic kidney disease.
Basics
Read the article on chronic kidney disease for a more comprehensive approach to the management of the condition. In this article, we will focus on discussing some important concepts regarding diuretics.
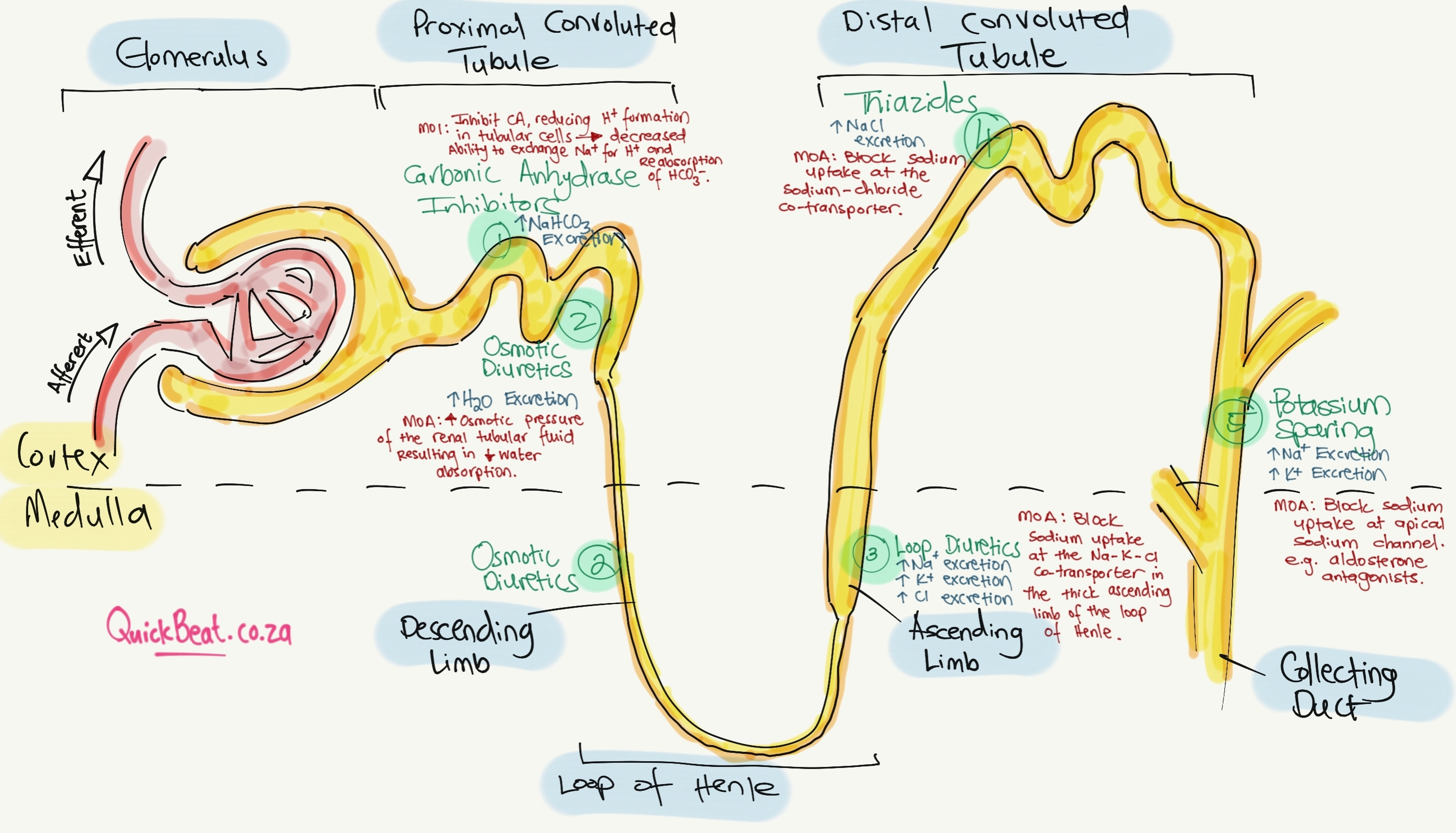
Thiazide Diuretics
- Thiazide diuretics are usually given to patients with an eGFR ≥ 30ml/min/1.73m^2.
- Common agents: Chlorthalidone, Hydrochlorothiazide (HCTZ), Indapamide, and Metolazone.
- Thiazide diuretics should usually be used in patients with CKD stages 1 to 3.
- In these stages, HCTZ should be started at a dose of 12.5 – 25mg/day and it may go up to 100mg/day.
- If the blood pressure remains controlled and there is no evidence of ECV expansion, then it is not necessary to change to a loop diuretic. However, at low a dose and reduced eGFR levels, there is insufficient diuretic potency. Therefore, at eGFR lower than 30ml/min/1.73m^2, thiazides are often changed to a loop diuretic.
- MOA: Acts in the distal convoluted tubule where it then inhibits the sodium chloride transport. Thiazide diuretics compete for the chloride binding site and this results in decreased absorption of sodium and chloride. When this occurs, this loss of sodium will result in an indirect reduction in plasma volume which in turn leads to an activation of RAAS (aldosterone secretion) and the further loss of potassium.
- Common side effects: Hypokalemia, hyponatremia, increased blood glucose, hyperuricemia (rise in uric acid).
- Thiazide diuretics and loop diuretics can be combined, especially for patients with ECF volume expansions and edema.
Loop Diuretics
- Loop diuretics are usually given to patients with an eGFR < 30 ml/min/1.72m^2.
- Common agents: Bumetanide, Furosemide, Torsemide.
- Furosemide may be started at dosages ranging from 20 – 80 mg/day. Furosemide may go up to a dose of 240mg/day.
- It is important to state that loop diuretics can be used at all stages of CKD.
- It is also important to know that loop diuretics are not as effective at treating hypertension as well as thiazide diuretics in stages 1-3. One of the reasons is that loop diuretics have a shorter duration of action. Loop diuretics also have a more erratic bioavailability. On average, 50% of a loop diuretic becomes absorbed when ingested (PO). However, this may range from 12% to 112%, this is in comparison with HCTZ which has a bioavailability of 60 – 80%.
- Thiazide diuretics and loop diuretics can be combined, especially for patients with ECF volume expansions and edema.
Potassium Sparing Diuretics
- Potassium-sparing diuretics should be used with some level of caution. This is because they increase the risk of hyperkalemia. Therefore, be careful in patients with an eGFR < 30, or with patients that are using medications that may cause hyperkalemia (ACE-I or ARBs).
- Common agents: Triamterene, Amiloride, Spironolactone, Eplerenone.
- Two types: Epithelial sodium channel inhibitors (Triamterene, Amiloride) and Mineralocorticoid receptor inhibitors (Spironolactone, Eplerenone).
- Should be used with caution due to an increased risk of hyperkalemia, especially in patients with an eGFR < 30. Therefore, may be used in CKD stages 1-3 but should ideally be avoided in stages 4-5.
- Spironolactone dosage ranges between 25 – 100mg/day. However, higher doses may not be possible due to the risk of hyperkalemia.
- Indications for their use: Persistent hypokalemia or resistant hypertension.


Made with ❤️ by QuickBeat
We are a small education agency that aims to provide medical education.
EXPLORE
SERVICES
CONTACT
- Pretoria North, Gauteng
- contact@quickbeat.co.za