Status Epilepticus
Basics
Definition
- A seizure that lasts more than 5 minutes or
- Recurrent seizures in close succession without the patient regaining full recovery of consciousness.
Etiology
- Infections of the CNS: Meningitis, encephalitis, intracranial abscess
- Metabolic abnormalities: Hypoglycemia, hyponatremia, hypocalcemia, hepatic encephalopathy, inborn errors of metabolism
- Cerebrovascular accidents
- Head trauma
- Drug withdrawal syndromes (alcohol, benzodiazepines, barbiturates)
- Hypoxia
- Hypertensive emergency
Management
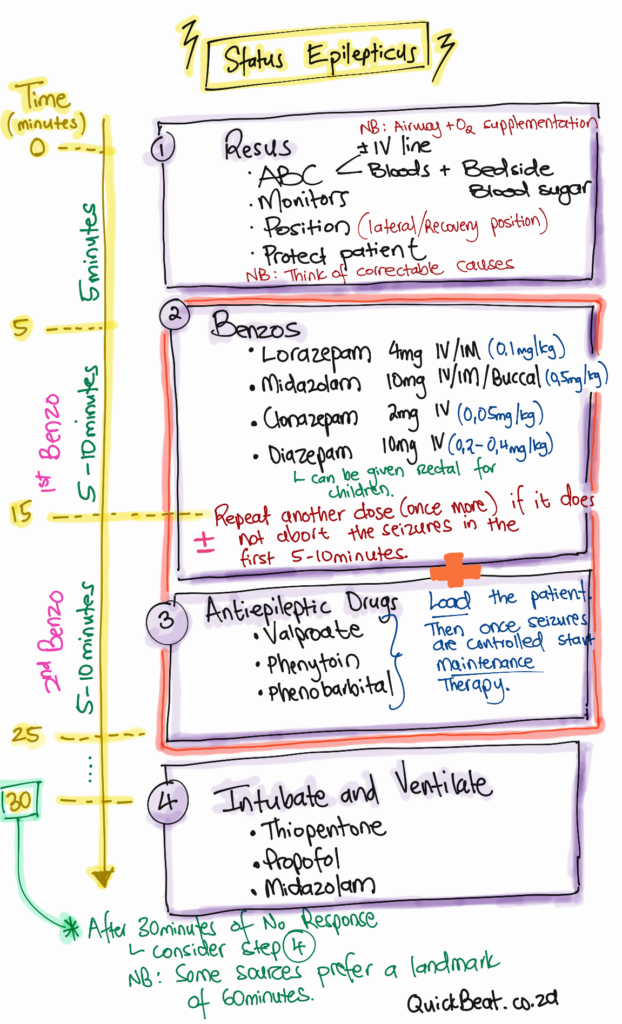
Step-Wise Approach
Take note that rapid sequence intubation may be necessary at any point during the management of the patient.
- Always remember to check for hazards and ask for help.
- Place the patient in a semi-lateral (recovery) position.
- Keep in mind throughout all steps: Protect the patient at all times: Ensure that the patient is in the correct type of bed with side rails, with little risk of falling. Do not insert any items in the patient’s mouth. This will cause more injuries. Position the head to maintain an open airway.
- This is an emergency, hence the need for your ABCs. Ensure that the airway is protected and provided the patient with supplementary oxygen.
- Attach monitors to monitor patient saturation, pulse, and blood pressure, and monitor the patient’s respiratory rate.
- Perform a bedside blood glucose test, if low treat with 50ml 50% Dextrose IV. If thiamine deficiency is a possibility (such as in alcoholics), administer thiamine before dextrose.
- Insert IV line, if possible.
- While inserting the IV line, take blood for investigations. Perform a blood gas to correct reversible causes if possible.
- Urea, Electrolytes and Creatinine, Glucose, Calcium, Magnesium, Phosphate, FBCs, blood/urine toxicology (if suspected), and anticonvulsants (if known to be on anticonvulsants).
- You may consider other studies based on the clinical presentation (liver function tests, inborn errors of metabolism, and coagulation studies).
- Stop the seizure with a benzodiazepine:
- Lorazepam 4mg IV/IM (0.1mg/kg) or
- Midazolam 10mg IV/IM/Buccal (0.5mg/kg) or
- Clonazepam 2mg IV (0.05mg/kg)
- Diazepam 10mg IV (0.2 – 0.4mg/kg). May also be given PR (Rectal) in children.
- You may repeat the dose after 5-10 minutes if seizures do not resolve following the first dose. If the second dose of benzodiazepines does not abort seizures, then the condition should be treated as a refractory status epilepticus and other agents will need to be used.
- Note: Hi, before you get too picky. Many institutions will have certain drugs over others and Diazepam is very common in public institutions – but it is not the “best”.
- Load and maintain: The patient requires an antiepileptic drug to be administered concurrently with benzodiazepines.
- Valproate: The loading dose is 15-30 mg/kg IV over 5 minutes. This agent may be repeated if there is no response. The maintenance dose is 50% of the initial bolus dose which is then given at an 8 hourly interval.
- Phenytoin:
- If valproate is not available AND If the patient is not already on phenytoin.
- The loading dose is 15-20 mg/kg IV as a slow infusion in normal saline over 30 minutes. Do not dilute phenytoin with dextrose water due to the potential of precipitation. The patient needs to be monitored continuously with an ECG. The phenytoin maintenance dose is 125 mg 8 hourly.
- Phenobarbital:
- If valproate is not available AND if the patient is not on phenobarbital.
- The loading dose is 20 mg/kg IV slowly in normal saline at around 100 mg/min. The Phenobarbital maintenance dose is 1 mg/kg 6 hourly.
- It is important to understand that if status epilepticus continues beyond the 30-minute landmark (others say 60 minutes), management should be escalated and patients should be ventilated using anesthetic doses of certain drugs. A neurologist should always be consulted.
- Anesthetic drugs: Propofol, Thiopentone, Midazolam.
- A lumbar puncture may be required at a certain point in the management of the patient. Rule out a state of raised intracranial pressure before proceeding with this investigation.
- Magnesium sulfate is indicated in a pregnant patient with eclampsia.
- A neurologist should always be consulted.
- All patients with status epilepticus require hospital admission.
Complications
The complications may be due to status epilepticus as well as due to the medications given to the patient. Time is important in the management of status epilepticus. The longer it takes to control the seizure the worst the patient’s outcome will be, especially the degree of cerebral hypoxia.
Medical Complications
Cardiac arrhythmia, respiratory failure, hypoventilation, hypoxia, aspiration pneumonia, pulmonary edema.
Neurological Complications
Progression to chronic epilepsy, permanent neurological damage due to prolonged status epilepticus (caused by the hyper-metabolic activity in regions of the brain which undergo a protracted abnormal electrical activity).
3. J., K.W.G. (2017) A guide to the management of common medical emergencies in adults. 11th edn. Johannesburg: Academy of Advanced Life Support.


Made with ❤️ by QuickBeat
We are a small education agency that aims to provide medical education.
EXPLORE
SERVICES
CONTACT
- Pretoria North, Gauteng
- contact@quickbeat.co.za