Disseminated Intravascular Coagulation
Basics
Causes
- Malignancy
- Sepsis
- Trauma
- Obstetric Events: Abraptio placentae, HELLP Syndrome, Amniotic fluid embolism.
- Other causes: Pancreatitis, snake bites, liver disease, transplant rejection, and transfusion reactions.
Presentation
This presentation varies depending on the clinical setting. However, these patients are prone to bleeding and hence will result in bruising, bleeding, and in extreme cases organ failure.
Pathophysiology
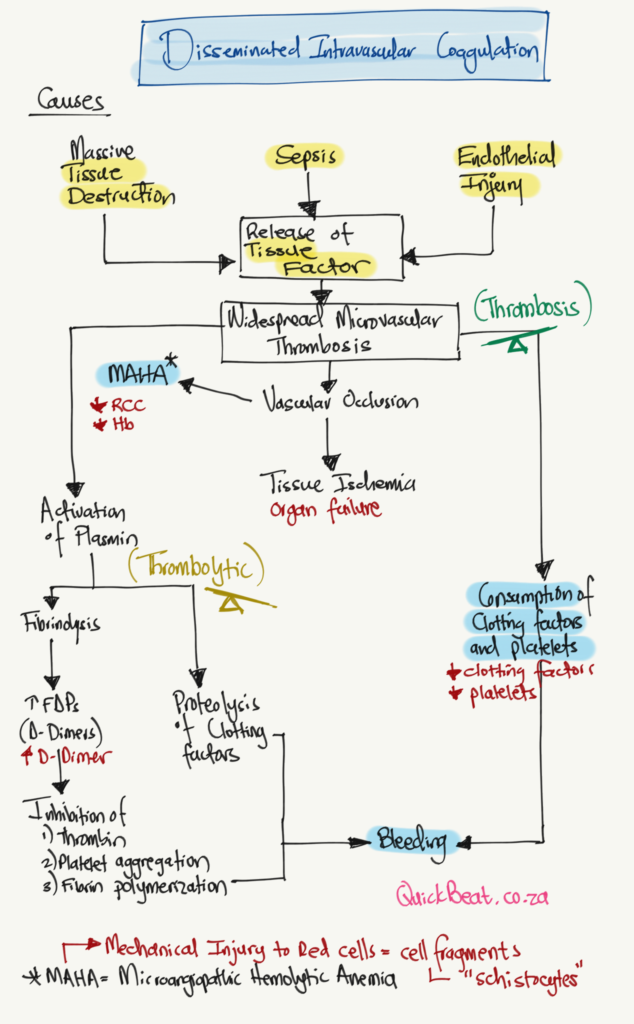
The diagram below shows a summary of DIC. There are several causes of DIC, however, most have a common pathway by activating the release of tissue factors. This results in excessive microvascular thrombosis. Microvascular thrombosis decreases organ perfusion. It also results in microangiopathic hemolytic anemia. This type of anemia results due to mechanical injury of the red cell as it passes through narrowed blood vessels. At this stage, we can see why the patient may develop anemia as well as organ failure.
As the disease continues, it results in the consumption of the clotting factors and platelets that are used in the formation of clots. We can appreciate this by seeing that the patient will develop thrombocytopenia as well as a deranged clotting profile. This means that the patient will begin to bleed.
At the same time, there is excessive thrombolytic activity (the clots are being broken down). This results in an increase in fibrin degradation products (D-Dimers).
Investigations
- Full Blood Count: Platelets are consumed, therefore low.
- Clotting Profile: PT time is prolonged, and aPTT is prolonged. Fibrin Degradation Products, also referred to as D-Dimer increased.
- Peripheral Blood Smear: This condition results in the formation of schistocytes.
Management
- Depends on the clinical condition.
- The target is to treat the cause.
- Replace the platelets only if they fall below < 50 x 10^9 platelets per liter for patients that are actively bleeding. However, any patient with platelets < 30×10^9/L should be transfused platelets if they are of high risk.
- Give the patient cryoprecipitate to replace fibrinogen (which is consumed during the process of coagulation).
- FFPs can also be given in order to replace the coagulation factors @ 15ml/kg.
- Others: The use of Heparin is controversial, usage of human-activated protein C has also been described in the literature.


Made with ❤️ by QuickBeat
We are a small education agency that aims to provide medical education.
EXPLORE
SERVICES
CONTACT
- Pretoria North, Gauteng
- contact@quickbeat.co.za